CDC
CDC
CDCとはCenters for Disease Control and Preventionの略称で、米国疾病予防管理センターなどと和訳されます。医療従事者であれば『CDCガイドライン』という言葉はよく耳にしています。使い捨て診療材料の交換頻度や、消毒方法などCDCを参考にしていることが多くあります。

[Link] Centers for Disease Control and Prevention (CDC)
CDCガイドライン
CDCからは様々なガイドラインが刊行されており、世界中で参照されています。
日本国の法律ではないので遵守義務はありませんが、医療界としての常識や水準として広く取り扱われています。
今回は”Guidelines for Environmental Infection Control in Health-CareFacilities”を参照します。
[Link] CDC: Guidelines for Environmental Infection Control in Health-Care Facilities
2.5パスカル要件
陰圧隔離室を作る際、2.5Paの差圧が必要という話題が良く出てきます。
その根拠はCDCガイドラインに由来します。
その記述は本文の”Recommendations — Air”(推奨事項:空気)の章の第4項”IV. Infection-Controland Ventilation Requirements for AII Rooms”(空気感染隔離室の感染制御および換気要件)に掲載されています。
※AIIはAirborne infection isolationの略
この項では、廊下より連続的に負圧を維持、その値は2.5Pa(0.01インチ水柱)とすること、定期的に、できれば毎日気圧をモニタリングし、結果を文書化すること、測定方法はマノメーターやスモークチューブが明記されています。

私たちは陰圧測定に『差圧計』を用いています。デジタルタイプなので精度には多少の課題があるものの、アナログ式より簡便に取り扱えますので、便利に使っています。
ピタリと2.5Paに合わせようとする場合は高精度の物が必要ですが、2.5Paを十分に超える差圧がある事を確認する目的で使用していますので、誤差については許容できると考えています。

|
デジタル差圧計
CDCガイドラインに沿って測定する場合の『Pa』(パスカル)であれば0~10000Paまで、1Pa単位で測定できます。分解能が1Paなので2.5Paの『0.5』は測定できません。 |
|
ソフトチューブ(内径4mm)
差圧を測定するために隣室へのチューブ敷設が必要です。ドア付近に差圧計を置く場合は3mもあれば足ります。差圧計のポートの1つは自室用に開放、もう1つのポートにチューブを差し込んで使います。私は金魚ポンプ用のチューブを使っています。 |
|
柴田科学 スモークテスターセット 080270-02
血圧計に付いていそうなゴム球をポンプすることで白煙が出てきます。ドア付近などで外から内へ空気が流入している事を確認します。逆流が確認される場合、陰圧が掛かっていない可能性がありますので改善策を講じます。 |
解釈
私たちが開発した簡易陰圧装置について、CDCガイドラインに完全準拠している訳ではありませんが、下表のような解釈により、CDCガイドラインの推奨事項に近づけることができると考えています。

| 給気量より排気量が多い事による陰圧、その圧力差は2.5Pa (0.01インチ水柱は約0.0254cm水柱) | ○ 強力なファンにより給気量を上回る排気が可能。実験において2.5Pa以上の差圧確認済 |
| きれいな空気から汚れた空気への流れ | ○ 給気量より排気量が多い事により実現可能 |
| 給気対排気の気流差125cfm (約3.54立米/min)超 | ○ HEPA無しで18立米/min (約635cfm)、HEPA装着で半減しても基準値を優に上回る排気量 |
| 新規・改修の部屋では毎時12回以上の空気入替、既存の部屋では毎時6回以上の空気入替 | ○ 排気量18立米/min、毎時1,080立米の排気が可能なため180立米を毎時6回排気(空気入替)可能 |
| 人の居ない外部への排気、または再循環する場合はHEPAフィルタ処理 | ○ ダクトで屋外に出せば外部排気、HEPA標準装着のため建物内での再循環使用にも対応 |
| 密閉された部屋で約0.5平方フィート(0.046平米)の漏れ | × 部屋の密閉は部屋の運用(ドア閉)や建築工事に依存します |
| モニタリング | × モニタリングには測定器の設置と記録が必要です |
In/OutのOutは制御下
私たちの開発した簡易陰圧装置は、文字通り簡易的に、陰圧を掛けるためのシステムです。
ある箱(部屋)があるとき、そこに陰圧を掛けるために必要な『負』のパワーを提供する事はできます。
しかしながら、箱の大きさ(部屋の容積)は私たちには決定できません。ユーザーの使用環境に依存します。
部屋を閉め切っているか、ドアが開けっ放しでないか、隙間風が入っていないか、それもユーザーの使用環境に依存します。
厳密にするのであれば前室を設け、陰圧室と他の部屋とが直接はつながらないようにし、前室で圧制御してドアを開閉し、陰圧室は隙間の無いように密閉処理された部屋にする必要がありますが、それでは簡易ではなくなります。
新興感染症で困っている医療機関や高齢者施設に、短納期で製品を納め、特別な工事なく使用してもらうために研究し、医療従事者の監修の下でCDCガイドラインに近づけた製品が私たちの開発物です。
ご不明な点は当社宛に、お気軽にご質問ください。
簡易陰圧装置だけではCDCガイドライン準拠は困難
前述の通り簡易陰圧装置はOut、すなわち排気して陰圧を掛ける事に特化しているがゆえに、部屋の容積が大きければ十分な陰圧はかかりません。
部屋のドアを開けっぱなしにした場合も同様で、廊下や隣室までが1つの空間としてつながってしまうため容積が大きくなり、陰圧がかからない可能性があります。
ある空間からウイルスを漏らさない事が目的なので、対象となる空間に適した装置の配備が必要です。
一般的な病室を想定して開発していますので、体育館のような所に1台配置しただけでは効果は期待できません。
装置を買って配置すればCDCガイドラインに準拠できる事はないと考えております。
私たちの目的は医療従事者や患者を守る事です。この簡易陰圧システムの開発は人道的面からスタートさせましたので、安易にCDCガイドライン準拠とは言いません。
正しく使って、正しく恐れる。私たちは医療機関や高齢者施設などに並走したいと思っています。
CDC 医療機関の環境に関する感染管理
Guidelines
”Guidelines for Environmental Infection Control in Health-Care Facilities”とは、医療施設における環境の感染管理のためのガイドラインと訳すことができると思います。
すなわち、患者ではなく環境に関する感染管理に特化したガイドラインです。

Guidelines for Environmental Infection Control in Health-Care Facilities
Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC)
医療施設における環境の感染監理のためのガイドライン
CDC(米国疾病予防センター)と医療感染管理実践諮問委員会(HICPAC)の推奨事項
Prepared by
Lynne Sehulster, Ph.D.
Division of Healthcare Quality Promotion National Center for Infectious Diseases
Raymond Y.W. Chinn, M.D.
HICPAC member Sharp Memorial Hospital San Diego, California
The material in this report originated in the National Center for Infectious Diseases, James M. Hughes, M.D., Director; and the Division of Healthcare Quality Promotion, Steven L. Solomon, M.D., Acting Director.
作成委員
リンセフルスター博士(国立感染症センターヘルスケア品質推進課)
レイモンドY.W. チン医師(HICPACメンバー/カリフォルニア州サンディエゴシャープメモリアルホスピタル)
このレポートは国立感染症センターJames M. Hughes局長(医師)とヘルスケア品質推進課Steven L. Solomon部長代理(医師)が発案したものです。
Summary
The health-care facility environment is rarely implicated in disease transmission,except among patients who are immunocompromised. Nonetheless, inadvertentexposures to environmental pathogens (e.g., Aspergillus spp. and Legionellaspp.) or airborne pathogens (e.g., Mycobacterium tuberculosis and varicella-zostervirus) can result in adverse patient outcomes and cause illness among health-careworkers. Environmental infection-control strategies and engineering controlscan effectively prevent these infections. The incidence of health-care–associatedinfections and pseudo-outbreaks can be minimized by 1) appropriate useof cleaners and disinfectants; 2) appropriate maintenance of medical equipment(e.g., automated endoscope reprocessors or hydrotherapy equipment); 3)adherence to water-quality standards for hemodialysis, and to ventilationstandards for specialized care environments (e.g., airborne infection isolationrooms, protective environments, or operating rooms); and 4) prompt managementof water intrusion into the facility. Routine environmental sampling isnot usually advised, except for water quality determinations in hemodialysissettings and other situations where sampling is directed by epidemiologicprinciples, and results can be applied directly to infection-control decisions.
This report reviews previous guidelines and strategies for preventing environment-associatedinfections in health-care facilities and offers recommendations. Theseinclude 1) evidence-based recommendations supported by studies; 2) requirementsof federal agencies (e.g., Food and Drug Administration, U.S. EnvironmentalProtection Agency, U.S. Department of Labor, Occupational Safety and HealthAdministration, and U.S. Department of Justice); 3) guidelines and standardsfrom building and equipment professional organizations (e.g., AmericanInstitute of Architects, Association for the Advancement of Medical Instrumentation,and American Society of Heating, Refrigeration, and Air-Conditioning Engineers);4) recommendations derived from scientific theory or rationale; and 5)experienced opinions based upon infection-control and engineering practices.The report also suggests a series of performance measurements as a meansto evaluate infection-control efforts.
概要
医療施設の環境は、免疫不全の患者を除いて、疾患の伝染に関与することはめったにありません。
それにもかかわらず、環境病原菌やまたは空中病原菌への不注意な曝露は、患者に有害な結果をもたらし、医療従事者への感染起こす可能性があります。
環境感染制御戦略とエンジニアリング管理は、これらの感染を効果的に防止することができます。
ヘルスケア関連の感染症と疑似アウトブレイクの発生率は、清掃係と消毒剤に適切な使用、医療機器の適切なメンテナンス、血液透析の水質基準、隔離室等の専門医療環境の換気基準の順守、施設への浸水への迅速な管理をすることで最小限に抑えることができます。
血液透析等の水質測定を除き、ルーチンでの環境測定は通常は推奨されません。環境測定は疫学の原則に基づいて行われ、その結果は感染対策に直接適用されます。
このレポートは、医療施設における環境関連感染を防止するためガイドラインと戦略をレビューし、推奨事項を提供します。
これらには、科学的理論または理論的根拠に基づく建築および設備の専門組織の推奨、連邦政府機関のガイドラインおよび標準の研究要件によってサポートされる証拠に基づく推奨、および感染管理とエンジニアリングの実践に基づく経験豊富な意見が含まれます。
レポートはまた、感染制御の取り組みを評価する手段として、一連のパフォーマンス測定を示唆しています。
(中略)
Recommendations — Air
推奨事項:空気
I. Air-Handling Systems in Health-Care Facilities
1.医療施設の空気処理システム
(中略)
II. Construction, Renovation, Remediation, Repair, and Demolition
2.建設、改修、修復、修理、解体
(中略)
III. Infection Control and Ventilation Requirements for PE rooms
3.保護環境室(陽圧室)の感染管理と換気の要件
(中略)
IV. Infection-Control and Ventilation Requirements for AII Room
4.空気感染隔離室の感染管理および換気要件
A.Incorporate certain specifications into the planning and constructionor renovation of AII units (1,34,100,101,104) (Figure 3).
Category IB, IC
A.空気感染隔離ユニットの計画と建設または改修に特定の仕様を組み込みます (1,34,100,101,104) (図3)。
カテゴリIB、IC
- Maintain continuous negative air pressure (2.5 Pa [0.01 inch water gauge])in relation to the air pressure in the corridor; monitor air pressure periodically,preferably daily, with audible manometers or smoke tubes at the door (forexisting AII rooms), or with a permanently installed visual monitoringmechanism. Document the results of monitoring (1,100,101).
Category IC (AIA: 7.2.C7, Table 7.2)
1.廊下の空気圧に対して、継続的な陰圧(2.5 Pa [ 0.01インチ水柱])を維持します。ドアにある差圧計または煙管(既存の空気感染隔離室の場合)、または常設された視覚的監視装置を使用して、定期的に、できれば毎日、気圧を監視し、モニタリング結果を文書化します(1,100,101)。
カテゴリIC (AIA:7.2.C7、表7.2)
- Ensure that rooms are well-sealed by properly constructing windows,doors, and air-intake and exhaust ports; when monitoring indicates airleakage, locate the leak and make necessary repairs (1,99,100).
Category IB, IC (AIA: 7.2.C3)
2.窓、ドア、吸気口、排気口を適切に構築して、部屋が十分に密閉されていることを確認します。モニタリングで空気漏れが示された場合は、漏れを特定して必要な修理を行います (1,99,100)。
カテゴリIB、IC(AIA:7.2.C3)
- Install self-closing devices on all AII room exit doors (1).
Category IC (AIA: 7.2.C4)
3.すべての空気感染隔離室の出口ドアに自動閉鎖装置を取り付けます(1)。
カテゴリIC (AIA:7.2.C4)
- Provide ventilation to ensure >12 ACH for renovated rooms and new rooms, and >6 ACH for existing AII rooms (1,34,104).
Category IB, IC (AIA: Table 7.2)
4.新設または改装された空気感染隔離室では12回/hr以上の空気入替、既存の空気感染隔離室では6回/hr以上の空気入替を確保するための換気を提供します(1,34,104)。
カテゴリIB、IC(AIA:表7.2)
- Direct exhaust air to the outside, away from air-intake and populatedareas. If this is not practical, air from the room can be recirculatedafter passing through a HEPA filter (1,34).
Category IC (AIA: Table 7.2)
5.吸気口や人の多いエリアから離れた外部に排気口を向けます。これが実用的でない場合はHEPAフィルタを通過した後、部屋からの空気を再循環させることができます(1,34)。
カテゴリIC (AIA:表7.2)
※.AIAとはAmerican Institute of Architects、アメリカ建築家協会
※.ACHとはair changes per hour、1時間あたりの空気入替(換気)回数
B. Where supplemental engineering controls for air cleaning are indicatedfrom a risk assessment of the AII area, install UVGI units in the exhaustair ducts of the HVAC system to supplement HEPA filtration or install UVGIfixtures on or near the ceiling to irradiate upper room air (34).
Category II
B.空気感染隔離エリアのリスク評価から、空気清浄のための補足的エンジニアリングコントロール(機械器具による制御)が示されている場合は、空調システムの排気ダクトに紫外線照射ユニットを設置して、HEPA濾過を補完するか、あるいは天井や天井近くに紫外線照射装置を設置して部屋上部の空気を照射します(34)。
カテゴリII
※.HVACとはheating, ventilation, air conditioning、暖房・換気・エアコンの総称
※.UVGIとはultraviolet germicidal irradiation、紫外線殺菌照射
C. Implement environmental infection-control measures for persons withdiagnosed or suspected airborne infectious diseases.
C.空気感染症と診断または疑われる人のための環境感染管理措置を実施する。
- Use AII rooms for patients with or suspected of having an airborne infectionwho also require cough-inducing procedures, or use an enclosed booth thatis engineered to provide 1) >12 ACH; 2) air supply and exhaust ratesufficient to maintain a 2.5 Pa (0.01-inch water gauge) negative pressuredifference with respect to all surrounding spaces with an exhaust rateof >50 ft3/min; and 3) air exhausted directly outside away from airintakes and traffic or exhausted after HEPA filtration before recirculation(1,34,105–107).
Category IB, IC
(AIA: 7.15.E, 7.31.D23, 9.10, Table 7.2)
1.咳を誘発する処置が必要になる空気感染患者またはその疑いのある患者には、空気感染隔離室を使用するか、以下の環境が提供できるようにせっけいされた密閉ブースを使用します。
1)12回/hr以上の空気入替ができる
2)毎分50立方フィート(約1.4立米)を超える排気速度で、周囲のすべてのスペースに対して2.5 Pa (0.01インチ水柱)の負圧差を維持するのに十分な給気および排気速度
3)換気口等から直接外部に排気、または再循環前にHEPA濾過して排気
(1,34,105–107)
カテゴリIB、IC
(AIA:7.15.E、7.31.D23、9.10、表7.2)
- Although airborne spread of viral hemorrhagic fever (VHF) has not been documented in a health-care setting, prudence dictates placing a VHF patient in an AII room, preferably with an anteroom, to reduce the risk of occupational exposure to aerosolized infectious material in blood, vomitus, liquid stool, and respiratory secretions present in large amounts during the end stage of a patient’s illness (108–110).
Category II 2.ウイルス性出血熱(VHF)の空中拡散は医療現場で文書化されていませんが、患者の病気のエンドステージに大量に存在する血液、嘔吐物、液体便、呼吸分泌物中のエアロゾル化された感染性物質への職業的曝露のリスクを減らすために、VHF患者を空気感染隔離室に、望ましくは前室を配置することを指示します(108-110)。
カテゴリII
a. If an anteroom is not available, use portable, industrial-grade HEPAfilters in the patient’s room to provide additional ACH equivalents forremoving airborne particulates.
a.前室が利用できない場合は、病室で携帯型の工業用HEPAフィルタを使用して、浮遊粒子状物質を除去するための追加の空気入替の同等物を提供します。
b. Ensure that health-care workers wear face shields or goggles with appropriaterespirators when entering the rooms of VHF patients with prominent cough,vomiting, diarrhea, or hemorrhage (109).
b.顕著な咳、嘔吐、下痢、出血のあるVHF患者の部屋に入るときは、医療従事者が適切な呼吸器を備えたフェイスシールドまたはゴーグルを着用するようにしてください(109)。
- Place smallpox patients in negative pressure rooms at the onset of their illness, preferably using a room with an anteroom, if available (36).
Category II
3.天然痘患者を発症時に陰圧室に配置します。可能な場合は、前室のある部屋の使用をお勧めします(36)。
カテゴリII
D.No recommendation is offered regarding negative pressure or isolationfor patients with Pneumocystis carinii pneumonia (111–113). Unresolvedissue.
D.ニューモシスチスカリニ肺炎の患者の陰圧または隔離に関する推奨事項はありません(111–113)。
カテゴリ Unresolved issue(未解決課題)
Maintain backup ventilation equipment (e.g., portable units for fans orfilters) for emergency provision of ventilation requirements for AII rooms,and take immediate steps to restore the fixed ventilation system (1,34,47).
Category IC (AIA: 5.1)
空気感染隔離室の換気要件を緊急に提供するために、バックアップ換気装置(ファンやフィルタ用のポータブルユニットなど)を維持し、固定換気システムを復元するための迅速な措置を講じます(1,34,47)。
カテゴリIC(AIA:5.1)
(中略)
Figure 3
図3
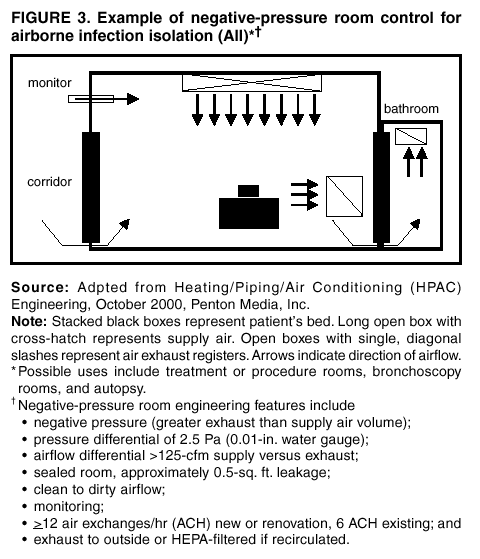
Figure3.Example of negative-pressure room control for airborne infection isolation (AII)
図3.空気感染隔離(AII)のための陰圧室制御の例
Source:
Adpted from Heating / Piping / Air Conditioning (HPAC) Engineering, October2000, Penton Media, Inc.
ソース:
暖房/換気/空調(HPAC)エンジニアリング (2000年10月、ペントンメディア社)から引用
Note:
Stacked black boxes represent patient’s bed.
Long open box with cross-hatch represents supply air.
Open boxes with single, diagonal slashes represent air exhaust registers.
Arrows indicate direction of airflow.
Possible uses include treatment or procedure rooms, bronchoscopy rooms,and autopsy.
注意:
積み重ねられた黒塗り部は、患者のベッドを表しています。
バツ印付きの長方形は、給気を表します。
一本斜線が付いた枠は、通風口(ガラリ)を表します。
矢印は気流の方向を示します。
考えられる用途には、治療室または処置室、気管支鏡検査室、および剖検が含まれます。
Negative-pressure room engineering features include
○negative pressure (greater exhaust than supply air volume)
○pressure differential of 2.5 Pa (0.01-in. water gauge)
○airflow differential > 125-cfm suply versus exhaust
○sealed room, approximately 0.5-sq. ft. leakage
○clean to dirty airflow
○monitoring
○>12 air exchanges/hr (ACH) new or renovation, 6 ACH existing; and
○exhaust to outside or HEPA-filtered if recirculated.
陰圧室のエンジニアリング機能には次のものがあります
○陰圧(給気量より多い排気量)
○圧力差2.5Pa (0.01インチ水柱)
○給気対排気の気流差125cfm超
○密閉された部屋で約0.5平方フィートの漏れ
○きれいな空気から汚れた空気への流れ
○モニタリング
○新規・改修の部屋では毎時12回以上の空気入替、既存の部屋では毎時6回以上の空気入替
○外部への排気、または再循環する場合はHEPAフィルタ処理
参照事項
評価カテゴリーについては下表を参考にします。
Category IA.
Strongly recommended for implementation and strongly supported by well-designedexperimental, clinical, or epidemiologic studies.
カテゴリIA
実装が強く推奨され、適切に設計された実験的、臨床的、または疫学的研究によって強くサポートされています。
Category IB.
Strongly recommended for implementation and supported by certain experimental,clinical, or epidemiologic studies and a strong theoretic rationale.
カテゴリIB
実装が強く推奨され、特定の実験的、臨床的、または疫学的研究と強力な理論的根拠によってサポートされています。
Category IC.
Required by state or federal regulation, or representing an establishedassociation standard. (Note: Abbreviations for governing agencies and regulatorycitations are listed where appropriate. Recommendations from regulationsadopted at state levels are also noted. Recommendations from AIA guidelinescite the appropriate sections of the standards.)
カテゴリIC
州または連邦の規制によって要求されるか、確立された協会の基準を表します。
注:必要に応じて、統治機関の略語と規制の引用がリストされています。州レベルで採用された規制からの推奨事項も記載されています。AIAガイドラインからの推奨事項は、標準の適切なセクションを引用しています。
Category II.
Suggested for implementation and supported by suggestive clinical or epidemiologicstudies, or a theoretic rationale.
カテゴリII
実施が提案され、示唆的な臨床または疫学研究、または理論的根拠によって裏付けられています。
Unresolved issue.
No recommendation is offered. No consensus or insufficient evidence existsregarding efficacy.
未解決の問題
推奨事項はありません。 有効性に関するコンセンサスまたは十分な証拠は存在しません。




